The GLP-1 Analog Revolution: Efficacy, Safety, and the Truth About Weight Loss (Beyond the "Ozempic Effect")
Are drugs like Ozempic or Mounjaro magic? We analyze the latest scientific evidence on GLP-1 analogs: efficacy comparisons (Tirzepatide vs. Semaglutide), safety profiles, and why muscle and nutrition are the missing link to avoid weight regain. A comprehensive guide based on systematic reviews and clinical studies.
Nuri El azem De haro
11/21/20255 min read

In recent years, the treatment of obesity has undergone a radical paradigm shift. What was once limited to general advice like "eat less and move more" now includes powerful pharmacological tools that are redefining what is possible in weight loss.
However, amidst the media hype and social media trends, it's easy to get lost. Are these drugs "magic"? What's the difference between one brand and another? And most importantly: Is an injection enough to be healthy?
In this article, we break down the science behind GLP-1 analogs, compare their efficacy based on the latest systematic studies, and explain why lifestyle remains the cornerstone of your health.
1. What Are GLP-1 Analogs and How Do They Work?
To understand these medications, we first need to look at our own digestive system. Naturally, when we eat, our body releases hormones called incretins. The most relevant ones are GLP-1 (Glucagon-Like Peptide-1) and GIP (Glucose-dependent Insulinotropic Polypeptide)².
These hormones have vital functions for metabolism:
They boost insulin secretion after eating to control blood sugar².
They act on the hypothalamus (the brain's control center) to suppress appetite and increase the feeling of fullness (satiety)².
They delay gastric emptying, meaning food stays in the stomach longer, which prolongs the sensation of fullness².
Current drugs are "mimetics" of these hormones: they mimic their biological action but with a much longer duration, allowing for potent control of hunger and body weight¹.
The New Generation: Dual Agonists
While drugs like Semaglutide mimic only the GLP-1 receptor, Tirzepatide represents an innovation by acting as a dual agonist (GLP-1 and GIP)²´³. This combined action is believed to enhance the metabolic and weight loss effects beyond what a single hormone achieves, improving both insulin sensitivity and fat mobilization³.
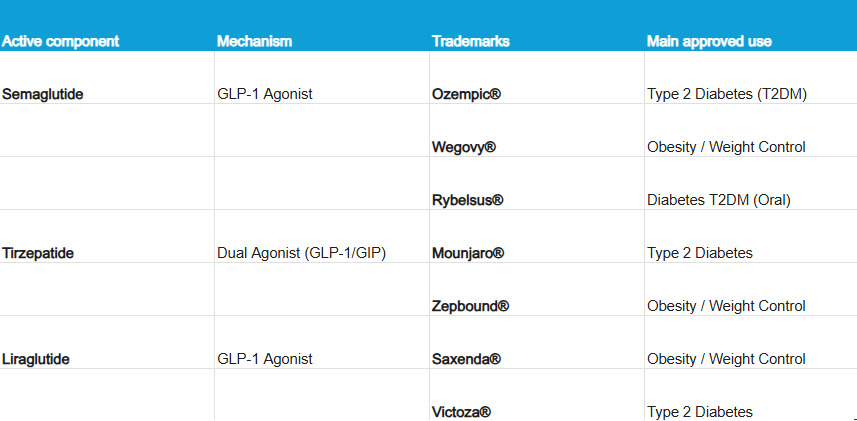
2. Names and Brands: Who's Who?
It's common to get confused with the commercial names. Here is a quick guide to distinguish them based on their active ingredient and regulatory approval (FDA/EMA), as dosages and devices vary depending on whether the goal is to treat diabetes or obesity²´³:
3. Efficacy Comparison: Which One Causes More Weight Loss?
The million-dollar question: Which drug is most effective? A recent systematic review, including over 41,000 participants across 22 randomized controlled trials, provides clear answers³.
Tirzepatide vs. Semaglutide
Studies consistently show that Tirzepatide (the dual agonist) tends to achieve greater absolute weight loss than Semaglutide:
In people without diabetes, Tirzepatide (15 mg dose) achieved an impressive weight reduction of 20.9% at 72 weeks³.
In comparison, Semaglutide (2.4 mg) achieved a reduction of 14.9% at 68 weeks in the same population³.
Both drugs significantly outperform Liraglutide (3 mg), which shows more modest efficacy but remains a valid, and possibly more economical, alternative after losing its patent³.
The "Diabetes" Factor
A crucial finding in the scientific literature is that people with Type 2 Diabetes lose less weight than those without diabetes, regardless of the drug used³.
With Tirzepatide (15 mg), diabetic patients lost about 9.5 kg (approx. 10–12% of body weight), compared to 20.9% in non-diabetics³.
This may be due to complex metabolic factors, entrenched insulin resistance, concomitant use of other medications, or genetic predispositions³.
4. Safety Profile: What Are the Risks?
No medication is without adverse effects. It is vital to know them to make informed decisions.
1. Gastrointestinal Effects (Most Common)
Up to 70% of patients experience digestive issues due to delayed gastric emptying². The most frequent include nausea (the number one in prevalence), diarrhea, vomiting, and constipation²´³. Generally, these effects are mild to moderate in intensity and occur mainly at the start of treatment or when the dose is increased ("titration")².
2. Pancreas and Gallbladder
There is a signal in studies regarding a potential risk of pancreatitis and biliary problems (like gallstones or cholelithiasis), especially with prolonged use and rapid weight loss². Although the direct causality of pancreatitis remains debated in clinical trials³, it is recommended to discontinue treatment if severe and persistent abdominal pain occurs.
3. Thyroid: Should I Be Concerned?
These drugs have been observed to induce C-cell tumors in the thyroid in animal models (rodents)². However, in humans, there is currently no sufficient evidence to support a clear carcinogenic risk². Still, they are contraindicated as a precaution if you have a family history of Medullary Thyroid Carcinoma or Multiple Endocrine Neoplasia type 2².
4. Mental Health
Recently, regulatory agencies like the FDA and the EMA investigated reports of suicidal ideation. The current conclusion after reviewing the data is that there is no proven causal link between these drugs and suicidal thoughts². Nevertheless, medical monitoring is advised, as obesity and chronic diseases themselves have a bidirectional relationship with mood disorders like depression².
5. The Missing Link: Lifestyle and Body Composition
This is where the science is clear: the drugs work by reducing appetite, but they do not educate about nutrition or ensure that what you lose is only fat¹.
The Danger of Muscle Mass Loss
When we lose weight quickly, the body also tends to "burn" lean tissue. Studies with Semaglutide showed that up to 39% of the weight lost was lean mass (muscle and bone)¹.
This is critical because muscle is the engine of your metabolism. Losing it increases the risk of sarcopenia (muscle weakness), reduces physical functionality, and facilitates the dreaded weight regain (rebound effect) by lowering the basal metabolic rate¹.
Structured Intervention vs. "General Advice"
It's not enough to say "eat healthy." To accompany these drugs, a Structured Diet and Physical Exercise Intervention (D-PE-I) is needed, which is very different from simple general lifestyle advice¹:
Protein is Key: It is recommended to increase protein intake to 1.0–1.5 g per kg of body weight per day (and even more in older adults) to protect muscle tissue during caloric deficit¹.
Strength Training: Aerobic exercise is good for the heart, but resistance training (weights, strength) is mandatory to preserve muscle function and bone quality while using the drug¹.
Malnutrition Risk: By eating much less due to appetite suppression, it's easy to develop vitamin and mineral deficiencies (Iron, B12, Vitamin D) if the diet is not professionally planned—a phenomenon known as "overfed but malnourished¹".
The Weight Regain Effect (The Rebound)
The data is clear: after stopping treatment, there is significant weight recovery if structural behavioral changes are not in place.
In studies with Semaglutide, two-thirds of the weight lost were regained within one year after withdrawing the drug¹.
With Tirzepatide, those who switched to placebo regained 14% of their weight, while those who stayed on the drug continued to lose or maintain their weight².
Conclusion: A Tool, Not a Magic Cure
GLP-1 analogs and dual agonists like Tirzepatide represent the most significant advance in the history of obesity treatment. Their efficacy is undisputed and superior to any previous pharmacotherapy³.
However, their use must be strategic and supervised. Pharmacology alone does not correct habits or ensure a healthy body composition. To prevent muscle loss, hidden malnutrition, and the rebound effect, treatment must always be accompanied by adequate nutrition (high in protein) and structured strength exercise¹.
Are you considering these treatments? Consult a specialist doctor who will not only prescribe the drug but also offer a comprehensive nutritional and physical follow-up plan. Your health goes far beyond the number on the scale.
References
[1] Minnetti, M., et al. (2025). "The Integration of Lifestyle Modification Advice and Diet and Physical Exercise Interventions: Cornerstones in the Management of Obesity with Incretin Mimetics". Obesity Facts.
[2] Fahim, S.A., et al. (2025). "Comparative safety and side effects of semaglutide and tirzepatide: Implications for clinical decision-making in obesity management". Biomedicine & Pharmacotherapy.
[3] Velji-Ibrahim, J., et al. (2025). "Efficacy and Safety of Glucagon-Like Peptide-1 Receptor Agonists for Obesity Management in Adults With and Without Type 2 Diabetes: A Systematic Review". Journal of Obesity.