The Definitive Guide to NSAIDs: Potency, Safety, and the Science Behind Pain Relief
A comprehensive review of the comparative efficacy and risks of the most common anti-inflammatories, based on the latest systematic evidence.
PAINKILLERS
Nuri El azem De haro
1/19/20264 min read


Pain is perhaps the most universal human experience and, simultaneously, the most complex to treat. To combat it, millions of people daily turn to Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). However, under familiar names like Ibuprofen, Naproxen, or Diclofenac, lie radically different pharmacological profiles.
Is the strongest drug always the best? Why do some destroy the stomach while others affect the heart? In this article, we analyze the most recent scientific evidence to answer these questions.
1. What exactly are NSAIDs and how do they work?
To understand potency, we must first understand the mechanism. NSAIDs work by blocking enzymes called cyclooxygenases (COX). There are two main types:
COX-1: Responsible for "maintenance" functions, such as protecting the stomach lining and aiding renal function.
COX-2: The "villain" that activates upon injury, producing the prostaglandins that cause pain and inflammation.
The "potency" of an NSAID usually depends on its ability to block COX-2, while its "adverse effects" typically stem from the unintended blockade of COX-1.
2. Relative Potency: The Efficacy Ranking
Thanks to network meta-analysis studies, which allow for the comparison of drugs never head-to-head in the same clinical trial, we now have a clear hierarchy.
The leaders in analgesic potency
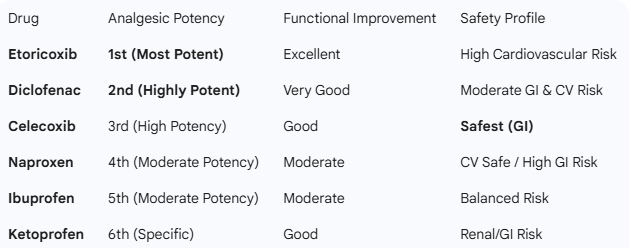
According to the most recent 2025 data for chronic pain such as osteoarthritis², Etoricoxib and Diclofenac (at doses of 150 mg/day) stand at the top. These drugs have shown a probability greater than 95% of being more effective than placebo and significantly more potent than their competitors in reducing joint pain and improving physical function².
The power of combinations in acute pain
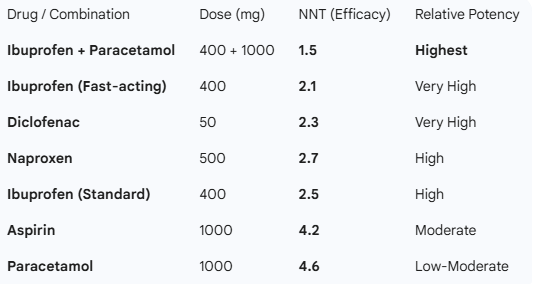
Interestingly, when discussing acute pain (such as a toothache or a sprain), the Cochrane review¹ reveals a surprising fact: the combination of Ibuprofen + Paracetamol is more potent than almost any NSAID alone. This synergy achieves a very low "Number Needed to Treat" (NNT), meaning it is extremely reliable¹.
The case for fast-acting Ibuprofen
Dosage isn't everything; formulation matters. Fast-acting ibuprofen (arginine or potassium salts) at 400 mg can be more effective and faster than a standard 600 mg tablet, proving that absorption speed is a crucial potency factor¹.
3. The Achilles' Heel: The Gastrointestinal System
The primary reason physicians limit NSAID use is the risk of gastric injury. This is where selectivity plays a vital role.
High Risk: Diclofenac and Naproxen have a higher tendency to cause gastric erosions if used long-term. By blocking COX-1, they leave the stomach without its protective mucus "shield," which can lead to ulcers or micro-bleeding².
The Benefit of Coxibs: Drugs like Celecoxib were specifically designed to avoid this issue. Being COX-2 selective, they "spare" the stomach. Studies indicate that the risk of serious gastrointestinal complications is drastically reduced with these agents².
Ketoprofen: Although a potent analgesic, some reviews suggest its gastrointestinal safety profile at controlled doses is more favorable than initially thought when compared to Diclofenac².
4. Other Adverse Effects and Cardiovascular Safety
It's not all about the stomach. NSAID use must be a constant balance between three pillars:
Cardiovascular Risk
This is the weak point of more modern and potent NSAIDs. Etoricoxib and, to a lesser extent, Diclofenac, have shown in recent studies a higher association with adverse cardiovascular events (high blood pressure, risk of thrombosis)². Conversely, Naproxen is often considered the "safest" for the heart, even if it is harsher on the stomach.
Renal and Hepatic Function
Continued use of any NSAID reduces blood flow to the kidneys. In patients with pre-existing conditions, this can cause fluid retention or kidney failure. On the other hand, excessive doses of paracetamol (often combined with NSAIDs) represent the leading cause of drug-induced liver toxicity².
5. How to Choose the Right NSAID? (Practical Conclusions)
Based on the combined evidence from Cochrane¹ and PLOS One², we can establish these golden rules:
For acute and fast pain: Look for combinations (Ibuprofen + Paracetamol) or fast-acting 400 mg Ibuprofen formulations¹.
For chronic inflammatory pain (Osteoarthritis): Etoricoxib is the most potent but should be monitored if you have high blood pressure².
If you have a sensitive stomach: Prioritize Celecoxib or always associate a gastric protector (like Omeprazole) if using classic NSAIDs for more than 3 days.
The minimum effective dose: Science is clear; increasing the dose above recommended limits does not linearly increase relief but does exponentially multiply the risk of adverse effects¹.
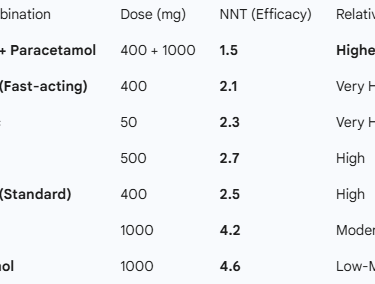
Table 1: Efficacy in Acute Pain
This table uses the NNT (Number Needed to Treat). A lower number indicates higher potency and reliability in achieving 50% pain relief.
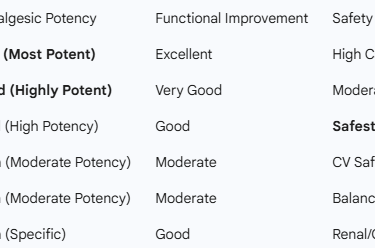
Table 2: Ranking in Chronic Pain & Osteoarthritis
Based on the probability of being the most effective treatment for pain reduction and physical function.
Final Note: This article is for informational purposes only. Before starting any treatment with NSAIDs, especially for prolonged periods, consult your physician to assess your personal cardiovascular and gastrointestinal risk.
References
¹ Moore RA, et al. (2015). Non-prescription (OTC) oral analgesics for acute pain - an overview of Cochrane reviews. Cochrane Database of Systematic Reviews.
² JiaoYi P, et al. (2025). Assessing the efficacy and safety of different nonsteroidal anti-inflammatory drugs in the treatment of osteoarthritis: A systematic review and network meta-analysis based on RCT trials. PLOS One.